This combination drug product is intended as a treatment for tension headache. Butalbital/acetaminophen/caffeine (Esgic, Floricet, Phrenilin Forte, Zebutal) is an inexpensive drug used to treat tension headaches. It is more popular than comparable drugs. it is available in multiple generic and brand versions. Generic butalbital/acetaminophen/caffeine is covered by most Medicare and insurance plans, but some pharmacy coupons or cash prices may be lower.

It consists of a fixed combination of butalbital, acetaminophen, and caffeine. The role each component plays in the relief of the complex of symptoms known as tension headache is incompletely understood.
The behavior of the individual components is described below.
Pharmacokinetics of Butalbital
Butalbital is well absorbed from the gastrointestinal tract and is expected to distribute to most tissues in the body. Barbiturates in general may appear in breast milk and readily cross the placental barrier. They are bound to plasma and tissue proteins to a varying degree and binding increases directly as a function of lipid solubility.
Elimination of butalbital is primarily via the kidney (59% to 88% of the dose) as unchanged drug or metabolites. The plasma half-life is about 35 hours. Urinary excretion products include parent drug (about 3.6% of the dose), 5-isobutyl-5-(2, 3-dihydroxypropyl) barbituric acid (about 24% of the dose), 5-allyl-5(3-hydroxy-2-methyl-1-propyl) barbituric acid (about 4.8% of the dose), products with the barbituric acid ring hydrolyzed with excretion of urea (about 14% of the dose), as well as unidentified materials. Of the material excreted in the urine, 32% is conjugated.
The in vitro plasma protein binding of butalbital is 45% over the concentration range of 0.5-20 mcg/mL. This falls within the range of plasma protein binding (20%-45%) reported with other barbiturates such as phenobarbital, pentobarbital, and secobarbital sodium. The plasma-to-blood concentration ratio was almost unity, indicating that there is no preferential distribution of butalbital into either plasma or blood cells.
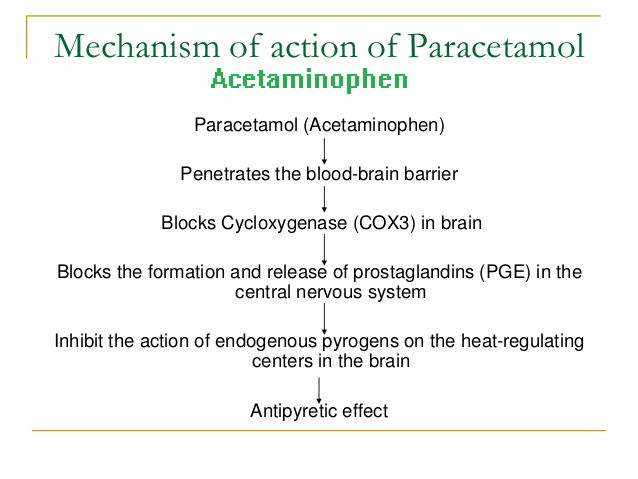
Clinical pharmacokinetics of Acetaminophen
Acetaminophen is rapidly absorbed from the gastrointestinal tract and is distributed throughout most body tissues. The plasma half-life is 1.25 to 3 hours, but may be increased by liver damage and following over dosage. Elimination of acetaminophen is principally by liver metabolism (conjugation) and subsequent renal excretion of metabolites. Approximately 85% of an oral dose appears in the urine within 24 hours of administration, most as the glucuronide conjugate, with small amounts of other conjugates and unchanged drug.
In therapeutic doses paracetamol is a safe analgesic, but in overdosage it can cause severe hepatic necrosis. Following oral administration it is rapidly absorbed from the gastrointestinal tract, its systemic bioavailability being dose-dependent and ranging from 70 to 90%. Its rate of oral absorption is predominantly dependent on the rate of gastric emptying, being delayed by food, propantheline, pethidine and diamorphine and enhanced by metoclopramide. Paracetamol is also well absorbed from the rectum.
It distributes rapidly and evenly throughout most tissues and fluids and has a volume of distribution of approximately 0.9L/kg. 10 to 20% of the drug is bound to red blood cells. Paracetamol is extensively metabolised (predominantly in the liver), the major metabolites being the sulphate and glucuronide conjugates.
A minor fraction of drug is converted to a highly reactive alkylating metabolite which is inactivated with reduced glutathione and excreted in the urine as cysteine and mercapturic acid conjugates. Large doses of paracetamol (overdoses) cause acute hepatic necrosis as a result of depletion of glutathione and of binding of the excess reactive metabolite to vital cell constituents. This damage can be prevented by the early administration of sulfhydryl compounds such as methionine and N-acetylcysteine.
In healthy subjects 85 to 95% of a therapeutic dose is excreted in the urine within 24 hours with about 4, 55, 30, 4 and 4% appearing as unchanged paracetamol and its glucuronide, sulphate, mercapturic acid and cysteine conjugates, respectively. The plasma half-life in such subjects ranges from 1.9 to 2.5 hours and the total body clearance from 4.5 to 5.5 ml/kg/min.
Age has little effect on the plasma half-life, which is shortened in patients taking anticonvulsants. The plasma half-life is usually normal in patients with mild chronic liver disease, but its prolonged in those with decompensated liver disease.
Caffeine
Like most xanthines, caffeine is rapidly absorbed and distributed in all body tissues and fluids, including the CNS, fetal tissues, and breast milk.
Caffeine is cleared through metabolism and excretion in the urine. The plasma half-life is about 3 hours. Hepatic biotransformation prior to excretion results in about equal amounts of 1-methylxanthine and 1-methyluric acid. Of the 70% of the dose that is recovered in the urine, only 3% is unchanged drug.